AFOLABI AO, AKINWONMI BA, DURODOLA AA
DEPARTMENT OF DENTAL SERVICES FEDERAL MEDICAL CENTRE OWO
INTRODUCTION
BURNING MOUTH SYNDROME (BMS) is a chronic intraoral burning sensation that has no identifiable cause either local or systemic.
It was first categorized as a distinct disease in 2004 by the International Headache Society, which defined primary BMS as “an intraoral burning sensation for which no medical or dental cause can be found. It often involves the tongue with or without extension t the lips and oral mucosa.
First described in the 1880s, this condition was further characterized in the early twentieth century by Butlin and Oppenheim as glossodynia (Painful tongue)
BMS has been referred to as glossopyrosis (burning sensation on tongue), Oral dysesthesia, Sore tongue, Stomatodynia (pain in the mouth), and Stomatopyrosis
EPIDEMIOLOGY
The prevalence is 15.8% in Nigeria and occurred mostly in young adults and females.
90% of the female patients are perimenopausal with typical onset from 3years prior to and 12 years post-menopausal age ranging from 27 to 87 years of age.
CLASSIFICATIONS
- Based on aetiology
Primary: no causative local or systemic disease can be founf
Secondary: Local or systemic factors/disease are present
Local factors
Oral mucosa disease/lesion
Fungal infection: candidiasis.
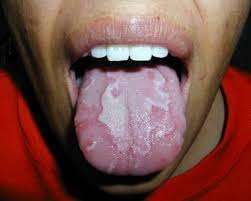
Other Conditions: geographic tongue, aphthous stomatitis, fissured tongue.
Trauma
Mechanical: Ill-fitting dentures, denture materials, sharp edges of restoration
Chemical: Abrasive toothpaste, aspirin use, acidic beverages.
Thermal: Hot or spicy food and beverages
Parafunctional Habits e.g Bruxism, and tongue thrusting
Salivary Gland disorders causing Xerostomia
Allergies: Zinc, cobalt, mercury, gold, and palladium, sodium lauryl sulfate.
Systemic factors: Several psychiatric diseases, depression and anxiety disorders, hypochondria and cancerphobia
Endocrine: peri/post -menopausal Patient patients due to lower levels of estradiol and increase levels of follicle stimulating hormone.
Diabetes mellitus: diabetic neuropathy, candidiasis
Hypothyroidism: xerostomia is a common feature. Regardless of whether the BMS is caused by thyroid hormone effect directly on oral mucosa or as a compilated caused by thyroid disease addresses the burning symptom
Immunologic etiology: Allergic reactions to dietary antigens such ascorbic acid, cinnamon, nicotinic acid, propylene glycol, and benzoic acid.
Autoimmune connective: tissue disorders such as sjogren’s syndrome and systemic lupus erythematosus, have also been associated
Nutritional deficiencies: vitamins B1, B2, B6, B12, folic acid, zinc deficiency, with patients reporting improved symptoms after zinc replacement theraphy
Drug-associated BMS: e.g ACE inhibitors and angiotensin receptor blockers
A potential relationship between smoking and development of BMS has also been described
- Based on the intensity of pain
Type 1 BMS (35%)
Patients having burning every day.
Burning sensation is absent on waking
This type may be linked to systemic disorders e.g. nutritional deficiencies and endocrine orders
Type 2 BMS (55%)
Patients having burning every day
Burning sensation is present on awakening and often makes falling asleep at night difficult.
These patients often report mood changes, alteration in eating habit and decrease dire to socialize
Type 3 (10%)
Intermittent burning sensation only present on some days
Burning sensation affects unusual sites e.g. floor of the mouth, buccal mucosa and throat.
These patients frequently display anxiety and allergic reactions, particularly to food additives.
PATHOGENESIS
BMS aetiologic remains under unclear and not totally understood. Recent studies have shown increasing evidence of neuropathic origin with central and peripheral nerve system involvement
CLINICAL FEATURES
Location: mostly affects anterior tongue followed by palate, lips and phsrync. However multiple sites may be involved.
Duration: 4 to 6 months
Character: burning
Severity: moderate to severe
Onset: usually spontaneous, however can be after participating event.
Associate factors: altered taste and dry mouth are the most common.
Some patients can be oligosymptomatic (pain and dysgeusia or xerostomia) or monosymptomatic (pain only). No visible disease in the oral mucosa
MANAGEMENT
History
Duration, intensity, location, aggravating and relieving factors of the pain
Taste alteration and dry mouth
Review of systems: GI and urogenital symptoms, headache, chronic fatigue, insomnia, mood changes, irritability, anxiety and depression
Medical history:
GERD, hypertension, hematological disorders, nutritional deficiencies, diabetes mellitus, thyroid disorders, Parkinson’s disease, Sjogren’s syndrome and other autoimmune diseases
CLINICAL EXAMINATION
Examination of dental hard and soft tissues
Inspection of oral mucosa and tongue for any pathological changes
Temporomandibular joint examination
Assessment of intraoral appliances
Investigations
Hematological assessment of nutritional deficiencies, (CBC count with RBC indices, serum albumin level, E/U/Cr)
Blood glucose levels (FPG, 2HPP)
Sialometry for salivary flow rate
Autoimmune markers: SLE, sjorgren syndrome, rheumatoid
Ari5thristis
Oestrogen and progesterone concentrations
Patch testing for special allergies
Oral cultures and scrapings to evaluate for a bacterial or fungal infection
Differential Diagnosis
Atypical facial pain
Atypical odontalgia
Trigeminal neuralgia
TMJ pain dysfunction syndrome
TREATMENT Based on type of BMS Secondary BMS treat the causative local or systemic disease withdraw offending medications
Primary BMS
Cure remains elusive despite attempts with different classes of in with medication. Treatment is aimed at managing as a type of chronic neuropathy. Management of primary BMS can follow (supportive Treatment)
Reassurance
Behavioral Modification
Pharmacological Approach (treating symptomatically)
REASSURANCE
It is important to provide patients with information on the nature of their condition and give reassurance.
This is essential as patient’s frustration and dissatisfaction is very common
They must also be informed of possible prolonged treatment Realistic treatment goal should be set as management is primarily Supportive and aimed at symptom reduction rather than symptom elimination.
BEHAVIORAL MODIFICATION
Patient is advised to desist from some activities that can induce or worsen patient’s symptoms. This includes:
Tobacco, Hot, spicy foods Alcoholic beverages Mouthwash that contains alcohol Products high in acids e.g., citrus fruits, juices.
HYDRATION
This tends to improve xerostomia symptoms. It is recommended that patient is advised to take plenty of fluids Chewing of sugar-free gums to keep the mouth moist
STRESS RELIEF
Stress has been associated with BMS However, managing stress and anxiety can improve the patients overall health
ENGAGING IN PHYSICAL ACTIVITIES
Encourage patient to engage in physical activities such as exercise, yoga, reading or other activities helps patient to relax Socially active
ORAL HYGIENE MEASURES
Use of alcohol-free mouth wash
Sodium lauryl sulphate free tooth paste
Keeping to strict oral hygiene measures
DIET ALTERATION
Avoid spicy foods and beverages such as citrus fruits, carbonated drinks, tomato sauces, and coffee. Acidic foods worsen BMS
PHARMACOLOGICAL APPROACH
Pharmacological protocols have not consistently proved to be predictable and effective in all BMS patients. Many Pharmacological agents administered topically or systemically, have been proposed to overcome the burning sensation.
Commonly used Pharmacological agents
- Topical Anesthetic agents: lidocaine spray/gel, benzocaine
- Atypical analgesic: Topical capsaicin cream
- Topical Benzodiazepine: clonazepam
- Mood-altering drugs: systemic benzodiazepines (diazepam clonazepam) and anti-depressants (TCA: amitriptyline)
FOLLOW UP
Because of the debilitative nature of this syndrome, as well as the frequently observed involvement of psychological disorders, BMS patients, particularly those resistant to treatment, should be offered regular follow-up from two to four times a month during the symptomatic period.
PROGNOSIS
Prognosis is poor as literature reports complete spontaneous remission in only 3% of the patients within 5 years after the onset.
CONCLUSION
BMS is a chronic medical condition with not fully established pathogenesis, it is highly complex, likely involving the central, peripheral, or combined neurological pathways. There is need for more research work on BMS.
REFERENCES
1. International Association for the Study of Pain (|ASP). Fact Sheet 2013. Burning Mouth Syndrome. http://www.iasp-pain.org. Accessed 8/6/21
2. Mock, David, Chugh, Deepikia. Burning Mouth syndrome. Int J Oral Sci 2(1):1-4
Join Our Pharmaceutical, Drugs and Health News Updates Group: https://chat.whatsapp.com/K0EecK8GeZf24d283IpAnS